


Diversity and inclusion should be at the heart of AI development
Interview with Dr Emma Karoune on this important topic

Emma Karoune speaking on a panel about Data Science Careers at AIUK 2025 (Turing)
Dr Emma Karoune is a Principal Researcher at The Alan Turing Institute, the UK’s National Institute for Data Science and Artificial Intelligence, working at the intersection of data science and health research. She is a strong advocate for democratising access to knowledge through open research practices, particularly the sustainability of research outputs and the implementation of equality, diversity, inclusion and access, to drive greater impact and equity in the development of AI. She is currently working to create and foster inclusive communities to accelerate clinical AI, including being a co-founder of the Clinical AI Interest Group and the AI for Women's Health Group.
Tell us about yourself and describe your journey so far as a data science and AI professional.
I’ve had a very non-traditional route into my current job having worked in multiple disciplines. I started my career training to be an archaeological scientist and have a PhD in Archaeobotany (the study of plant remains from archaeological and palaeocological deposits) from University College London. I then worked in science education (teaching, examining, training, leading) and finally came back into academia to focus more on open research and data science. This background has given me a variety of valuable experiences and skills.
I’ve heard this type of career is called episodic - where you are very adaptable, curious and like the challenge of working in new fields. That definitely does sum me up but I also like to think of myself as a generalist. I focus on what transferable skills I have, such as research methods, technical skills, soft skills, and leadership, and how I can apply them across different areas. This mindset is very suited to working in data science and AI because it is such a new and rapidly developing field. New roles and opportunities are emerging all the time and you constantly need to problem solve to get over challenges and be creative to develop new avenues of research.
I also think that there is no traditional route into research, particularly for those working in data science or related roles. Few people actually do the traditional linear climb from PhD student to professor. Many people now working in data science and AI have not completed any formal qualifications in computer science or data science and have just picked up the technical skills and knowledge along the way.
There is a growing need in data science and AI for experts with socio-technical skills. By this I mean people that understand the technology but can consider and bring in diverse people and cultures, and the infrastructure needed to make that technology relevant and usable for society. This involves having different types of skills, both technical skills, and soft skills such as collaboration, communication and engagement skills. This is the type of work that I now focus on — bringing the right people together, enabling them to work together by removing barriers and making sure that they are considering societal needs during the development of any technology.
How has your experience shaped your approach to health tech innovation?
Although being a researcher is hugely interesting and rewarding, there are negative aspects to this career. For example, it’s often very precarious and highly competitive. Added to this, data science and AI is still a male dominated sector with a lack of women in senior leadership roles. This can make it difficult to be a woman in this space as these elements are often fighting against you or deterring you from career progression.
I have been lucky to benefit from the support of some amazing female leaders. The Turing Way Community (an open source project working to make data science more reproducible, ethical and collaborative), led by Dr Kirstie Whitaker and Dr Malvika Sharan, has really supported me in my career progression. The Turing Way leaders have demonstrated compassion and inclusivity to ensure everyone has the opportunity to step up into leadership positions in the community. This has shown me that if you take away barriers to participation by working hard to be as inclusive as possible it allows anyone to step forward.
I’ve also been part of Fellowships through the Software Sustainability Institute and ELIXIR-UK where considerable thought and intention has been put into making their networks inclusive. These experiences have shaped how I want to approach working in data science and AI.
How have you use technology to solve the healthcare problem which you are most passionate about?
I therefore approach data science and AI research with equality, diversity, inclusion and accessibility as a core aspect of my work. This is to ensure that all the right voices can be, and are, involved in any research I do. If this is not an intentional approach, the technology or solution that is developed won’t address the right need or be the right solution for those it is being developed for.
I lead a team of Research Community Managers at The Alan Turing Institute who work across different data science and AI focused communities. Our core aim is to foster a collaborative environment where a diverse research community can access the socio-technical infrastructure and participatory processes they need to actively engage, get recognition and build shared agency over the research being done. In health-related research, this means coordinating a large range of voices and thinking about how they can work together with each person bringing a different level of understanding and insight.
Truly embedding patients and the public in data science and AI research is still rare, and difficult, particularly due to the level of technical understanding that is needed to be able to meaningfully engage in the research. I am particularly proud to have been involved in the AI for Multiple Long Term Conditions Research Support Facility (AIM RSF) led by the Turing in collaboration with Swansea University, the University of Edinburgh and the University of Oxford. We were a unit of data science experts, funded by the National Institute for Health Research (NIHR), tasked to bring together the eight research consortia across the AIM programme. We played a pivotal role in developing data standards, disseminating best practices, and fostering a vibrant community encompassing researchers, patients, and the wider public actively engaged in AI for multiple long-term conditions (MLTC) research.
Where we really got things right in our approach to working with patients and the public was removing barriers to contribution. This meant creating equity such as increasing contributors knowledge of what data science and AI are, paying patient contributors for their time, providing accessibility funds to allow them to be involved in our conferences and also training researchers in how to interact and properly involve patients in their research.
You can find out more about our work in AIM RSF in our three case studies about data access, building capacity in health data science and engaging with representative groups.
What role do you see AI and other such digital innovations playing in the future of Women's health?
A community that I currently co-lead is the Clinical AI Interest Group. This group has grown exponentially in popularity since its creation in 2022 and now has a membership of over 1500 consisting of clinicians and wider healthcare professionals, data research professionals, regulators and tech workers. We have developed supra-interest groups in clinical specialties to bring together our members in a more focused manner. As well as monthly online meetings of our main group, the supra-interest groups meet regularly to share research, have discussions and start new collaborations. This is leading to great things such as research papers, events and now the AI for Women’s Health Group being recently recognised in the 2025 AI Visionaries initiative from Health Innovation Kent Surrey Sussex (KSS) and the Department for Health and Social Care (DHSC).
Bianca Schor (AI Researcher at Amsterdam’s UMC), former Turing enrichment student, is responsible for the idea of the AI for Women’s Health Group and I initially supported her in setting up the group, which now has two more co-organisers - Annalisa Occhipinti (Associate Professor at Teesside University) and Kristin Caolo (PhD Candidate at University of Cambridge). We are an interdisciplinary community interested in advancing women's health and how to leverage AI to do so. We run regular online meetings with a wide range of speakers and topics.
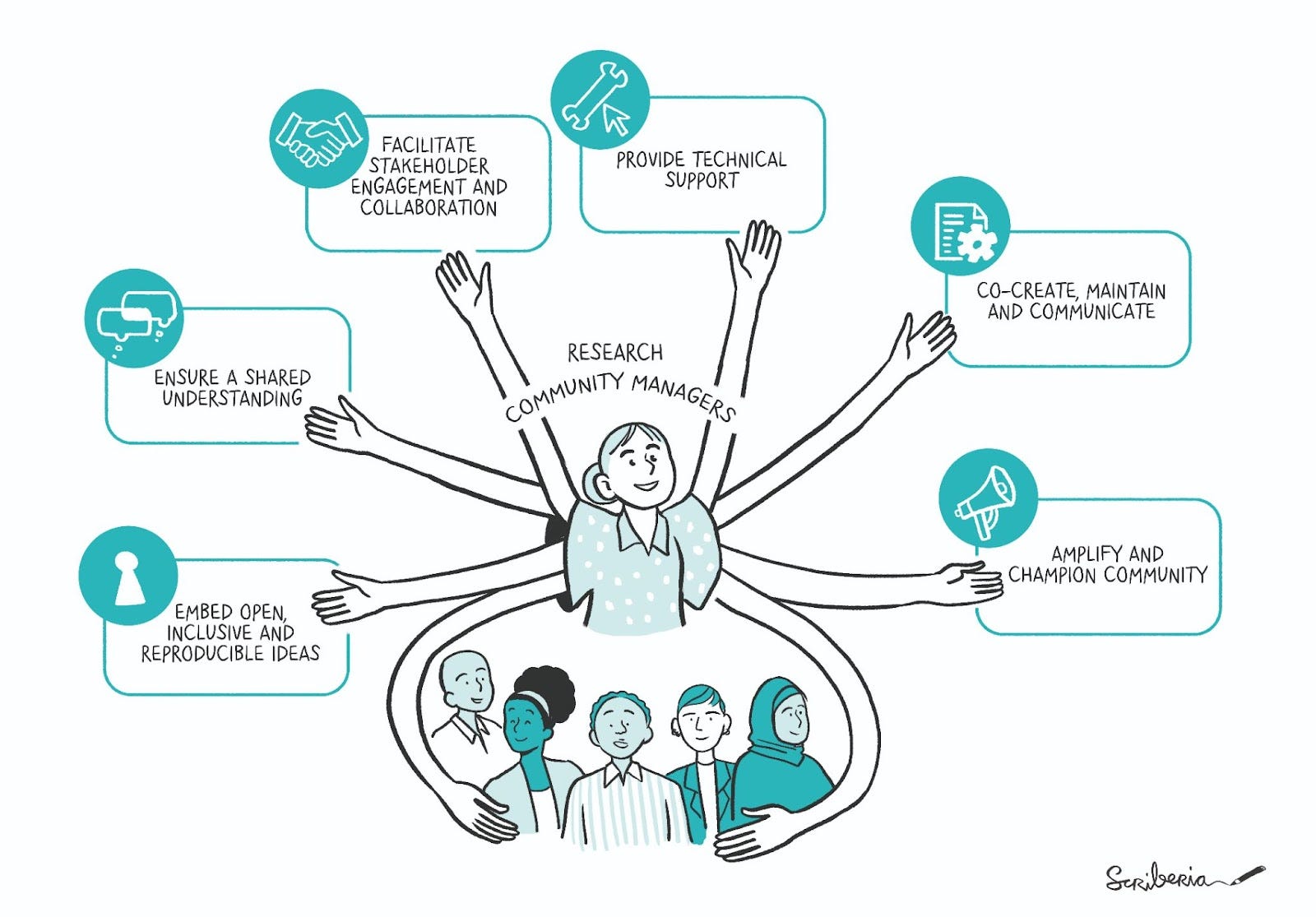
Research Community Manager - Courtesy of The Turing Way Community. This illustration is created by Scriberia with The Turing Way community, used under a CC-BY 4.0 licence. DOI: 10.5281/zenodo.3332807
Myself and the other co-organisers of the AI for Women’s Health Group were really overwhelmed and happy to have been recognised as part of the 2025 AI Visionaries initiative. We joined the other AI Visionaries and a whole host of people that work in the Clinical AI space at the first ever Responsible AI: Women and Healthcare Conference 2025, on the 30th January at the Royal College of Obstetricians and Gynaecologists. This was a highly attended event with key leaders from the NHS and government giving talks.
The conference was opened by Professor Erika Denton (National Director for Transformation, NHS England) and Dame Lesley Regan (Women’s Health Ambassador, His Majesty’s Government) who both highlighted that women make up the majority of our population, (51%), but they are being let down by our healthcare system. This is due to a lack of data, or biased data, and generally a lack of research on women, from basic science to the development of new practices and drugs, to informing clinical care.
This critical gap identified in healthcare means women’s health issues often go overlooked, with a striking 60% of UK women reporting their medical concerns aren’t taken seriously.
A recent report estimates closing this gap could potentially boost the global economy by $1 trillion annually by 2040, and states that although women live longer, they spend more of their lives in poor health. At the conference it was said that the UK could save £36 billion a year in the NHS by closing this gap - not a small amount!
Takeaways that emerged from the conference were:
It all comes back to data - women are not included in health data for many reasons and therefore won’t be properly represented in research and any algorithms made as
a result.
More investment is needed in women's health research, whether this is for AI or not! Women are not a minority and closing the healthcare gap would allow them to be more active members of society and ultimately save us billions each year.
Support more diverse leaders including women for greater health equity - we need to promote women and people from other under-represented groups in AI to be the future technological leaders to close this healthcare gap.
Clinician and patient voices should be at the heart of technological development - as technology developers we need to actually answer clinical challenges, not just want to make the next technological advance.
I was encouraged to see that the themes emerging from the conference were well aligned with my own research focuses, in particular the need to include the right stakeholders in the research and support women to lead AI research. I want to encourage women already working in data science and AI to create inclusive spaces to allow young women, and people from other underrepresented groups, to step forward into leadership as this is how we are going to drive forward technology that serves all of society.
Thanks to the other co-organisers of the AI for Women’s Health Group - Bianca Schor, Kriston Caolo and Annalisa Occhipinti - and the Clinical AI Interest Group - Alisha Davies, Nick Fuggle and Joe Alderman - for all their hard work to drive these groups forward. Thanks also to Cass Gould Van Praag (Gender Equality Network Group Co-Chair) and Daisy Brown (LGBTQ+ Equality Network Group Chair) for providing inclusion advice for this post.
Terminology
I use the term “women” in this post and this research community to refer to people who are assigned female at birth. I acknowledge that not all women are assigned female at birth and that not all those who are assigned female at birth identify as women. The use of the term “women” in this context is used to highlight the lack of data, research and disparity in healthcare when compared to people identified male at birth. A future activity of the AI for Women’s Health group may be to expand the scope of interest to campaign for resourcing to address the specific medical needs of transgender women, transgender men, non-binary and gender fluid people, acknowledging the systemic biases in healthcare that these groups face (see Trans inclusive healthcare for more coverage of this topic).
 | A guest post by
|

