
My hypothesis is that the massive, population-wide lowering of cholesterol among the American public leading up to 2019 set the stage for vulnerability to the novel pathogen SARS‑CoV‑2, the virus that causes COVID-19. This weakening of people’s defenses turned what could have and should have been a nuisance common cold into a very difficult and dangerous illness for those who were older, obese, or who suffered from multiple chronic illnesses.
Statin drugs lower cholesterol, especially what is called “bad” low-density lipoproteins (LDL) that carry cholesterol to our cells. Statins have been among the most common prescriptions in the United States for decades. In 2013, the American College of Cardiology and the American Heart Association recommended that everyone between the ages of 65 and 75 who were at elevated risk of cardiovascular disease (nearly everyone) be prescribed a statin drug. Then, by 2019, statins were a $10 billion market, and over 92 million people—35 percent of the U.S. population—mostly older adults, were taking statin drugs. This number was a threefold increase from the previous decade. By 2020, the United States ranked sixth in the world in per capita statin use.
So in 2019, the American public was about as saturated with statins as we had ever been.
Story continues below advertisement
The perhaps unintended result was that statin saturation rendered many seniors vulnerable to devastating outcomes from an infectious illness such as COVID-19. That cumulative vulnerability, which peaked in 2019, likely represented the lowest point of collective immune capability, and those extremes crested right before COVID-19 hit, as I will show in this article.
Statin drugs lower a person’s cholesterol, and cholesterol is not a luxury but rather a necessity for forming the vitamin D molecule—the conductor of the symphony, so to speak, of the human immune system.
Three organs are involved in your vitamin D production: first, the skin, then the liver, and finally, the kidneys. This is to take vitamin D to where it’s fully activated for its role as the executive director of all of a person’s immune function, as in the diagram below.
Vitamin D is the gateway nutrient to the proper functioning of the rest of the immune system, and was especially crucial in battling COVID-19, as I showed in over 130 study references to vitamin D’s role against COVID-19 and other infectious illnesses—in both treatment and prevention—in my 2021 book, “The Defeat of COVID.” Both those with higher blood lab values of vitamin D and those who supplemented vitamin D vanquished COVID-19 much more readily—with respect to lower hospitalization and lower deaths—than those who avoided vitamin D or who were deficient in it. Hundreds of studies and meta-analyses have shown this to be the case: Vitamin D preemptively defeats COVID-19 and other respiratory and viral illnesses—especially when dosed, or produced in the skin from sunlight, early and regularly.
Story continues below advertisement

Setting the Stage for COVID Vulnerability
The average age at death due to COVID-19 was 81, which was two to three years beyond the U.S. life expectancy at that time, so COVID-19 very disproportionately affected seniors, especially those with obesity, Type 2 diabetes, smoking, and more than two comorbidities.COVID morbidity and mortality in the United States far exceeded worldwide numbers. The United States has 4 percent of the world’s population, but 33 percent of the world’s deaths from COVID-19. The United States also had by far the greatest number of diagnosed COVID-19 cases of any country—over 103 million—followed by India at 44 million. The United States had 1.1 million deaths attributed to COVID-19.
Story continues below advertisement
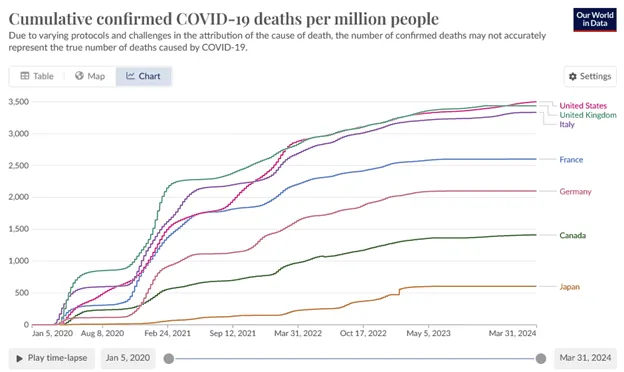
Our World In Data shows the United States with more COVID deaths per capita than any country, nearly tied with the UK and Italy, as of March 2024.
Deaths and morbidity from COVID-19 were augmented due to the medical system’s ignorance and incompetence about cholesterol, which led over recent decades to the proliferation of statin drug prescriptions. This may have been influenced by a tendency among the prescribers to turn away from uncomfortably unprofitable lines of inquiry, such as, “How can cholesterol be bad when it has so many functions in the body?” Upton Sinclair once said, “It is difficult to get a man to understand something when his salary depends on not understanding it.” The statin gravy train was just too lucrative, and it was just too inconvenient to question the “cholesterol bad, statins good” mantra if you were in the industry.
Therefore, it was much easier to demonize a devil-molecule in the body and to sell a drug to rid the vilified substance than to examine if the devil-molecule was a threat to health in the first place.
Story continues below advertisement
So then we need to ask: “What does cholesterol do, and how does it work?”
What Does Cholesterol Do?
Cholesterol is essential to every cell in the body. The liver makes it when we don’t get enough from food; the liver makes about 75 percent to 80 percent of our cholesterol, with the other 20 percent coming from food, which is one indication of how badly we need it.The cholesterol carried by the LDL cholesterol (so-called “bad cholesterol”) is particularly valuable because it is the major vehicle by which cholesterol is carried to the cells. When cholesterol arrives there, it forms an essential component of cell membranes. For humans as well as other mammals—including those mammals who live on fries and chips, as well as those foraging in nature—cholesterol is such an important fat in mammalian cell membranes that it makes up about 30 percent of the lipid bilayer.
Cholesterol is what keeps our cell membranes supple and strong while enabling the essential signaling transduction that life requires. Nuclear magnetic resonance imaging has shown that cholesterol is required for the essential flow of signaling proteins. Without signaling among our cells, the body would have no means to sustain life; conversely, one definition of death might be the end of cooperative interaction and signaling among the cells of the body.
The neurons are cells that are even more dependent on cholesterol than most, and cholesterol is abundant throughout the central nervous system. When cholesterol is lowered, damage to cognition and memory has been seen to follow—in mice as well as in humans. Observations of Framingham Heart Study participants showed “a significant positive linear association between [total cholesterol] and measures of verbal fluency, attention/concentration, abstract reasoning and a composite score measuring multiple cognitive domains.” Do you suppose your older relatives would have appreciated learning about that finding before taking such a drug? Deficiency of cholesterol has also been seen in Parkinson’s disease: “Higher cholesterol levels are associated with a lower risk of Parkinson’s disease.”
Story continues below advertisement
Cholesterol is necessary to digest foods, as it is the main source material for bile acid production. Bile acids facilitate the absorption of nutrients, and they act as a detergent to break down fats, so they are the main way the liver catabolizes dietary fats and cholesterol.
Cholesterol is the necessary source for our reproductive hormones, testosterone, progesterone, and estrogen, as well as our glucocorticoids and mineralocorticoids. This source is made available in the gonads in youth, and in the adrenal glands throughout life. So cholesterol is required for adequate adrenal function.
Finally, and most pertinently to the topic of this paper, cholesterol is required for vitamin D synthesis, which is needed for life after COVID-19 and victory over other pathogenic microbes, as discussed above.
Story continues below advertisement

How Statin Drugs Work
Statin drugs target and inhibit—really, they poison—the enzyme necessary to form cholesterol. The enzyme is HMG CoA reductase (3-hydroxy-3-methylglutaryl coenzyme A reductase) in the blood and the liver. Without this enzyme, we cannot produce cholesterol. Statins are especially effective at reducing LDL cholesterol, which has been called “bad cholesterol” so ubiquitously that both doctors and patients have come to accept this as true. The trouble is that it’s not true.Dr. Aseem Malhotra is the UK’s most recognized cardiologist. He says this about LDL cholesterol: “It’s a useless biomarker in terms of predicting someone’s risk of heart disease and therefore we shouldn’t obsess about lowering it.” His book “A Statin-Free Life” argues that statins are not at all adequate for preventing heart disease.
Poisoning is a strong word, and it should probably be used sparingly. The destructive effect of statin drugs on the enzyme HMG CoA reductase not only has the effect of reducing the production of cholesterol, especially LDL cholesterol but also of Coenzyme Q10 (CoQ10). This, in turn, reduces flow to each of the downstream pathways.
The problem with reducing CoQ10 is that doing so impairs mitochondrial function because CoQ10 is key to the electron transport chain, which is required for ATP production to keep the body alive. So CoQ10 and mitochondria generally are also necessary for life and thriving. The loss of CoQ10 from statin prescription is the most likely explanation for the frequent muscle pain and fatigue suffered by those taking statins. That is, when your low CoQ10 fails the needs of your mitochondria, then your mitochondria fail the needs of your muscles, including the heart, which is nearly all muscle.
The Cochrane Heart Group writes: “The severity of heart failure correlates with the severity of coenzyme Q10 deficiency.” You see, when you attempt to selectively poison one biochemical pathway, such as the cholesterol-forming pathway, you end up with rather nasty unintended consequences from damage to the various parallel tributaries downstream.
Not all of this damage was lost on the people taking statin drugs, and so when inevitable side effects accumulated, compliance with prescriptions turned out to be low. Statins are such a hard-to-tolerate class of drug that 75 percent of people prescribed statins were no longer taking them a year later.
Everything You Were Told About Statins and Cholesterol Was Wrong
A reader who is remotely familiar with my previous articles or books knows that to describe me as a medical contrarian is an understatement. Case in point: My total cholesterol, last time measured, was 289, and that is where I want it, especially now in my senior years, due to extensive, not deficient, study of cholesterol’s vital roles in the body.The four-decade global campaign to curb heart disease by lowering cholesterol through diet and drugs has sadly failed.
However, most conventional medical providers are convinced that cholesterol is the body’s arch-enemy molecule, particularly the feared LDL and very-LDL, for being the alleged couriers of heart disease. Even while admitting that only one in eight randomized trials of statins’ effect on mortality showed decreased all-cause mortality, the American Medical Association, the American Heart Association, and all other mainstream medical organizations repeat and reinforce the belief among themselves, as they do to the believers among the rest of the medical profession, the media and the public. Cholesterol is a problem molecule, and your job is to reduce it.
Researchers Paula Byrne, Maryanne Demasi, Mark Jones, et al., did a systematic review and meta-analysis of 21 statin trials involving over 140,000 subjects. They found no consistent relationship between lowering LDL-C and death, heart attack, or stroke following statin therapy.
Before the COVID-19 vaccines and their abysmal efficacy and hazards, statin drugs had the worst benefit-to-risk ratio of any class of drugs. Even when viewed in the most favorable light, even among studies that were already biased pro-statin, it was found that, over five years, statins could, at best, offer three to four additional days of life. That’s it; in the most favorable circumstances: three or four days more over a five-year period.
Statin makers have never made their data available to the public, and regulators have helped them hide it from outside observers.
Clinicians have complained for many years about their patients’ reactions to statins. One writes: “Ever since the statins hit the market, colleagues and I began observing case after case of individuals who lost sensation in their body, developed muscle pains, or had cognitive decline set in once they started the statin, which immediately resolved once they stopped the statin.”
“Statins are the biggest fraud in modern medicine,” wrote Dr. David Brownstein on his blog in 2015.
The Statin Craze
The statin craze of our era has reduced people’s cholesterol, which in turn took away people’s ability to make vitamin D in the skin upon sun exposure. (A possibly separate issue is that decades of propaganda against sunlight may be due to the fact that sunlight is free and has no shareholders, but there is money to be made from the sale of sunscreens.) So now we have a population that threw away their cholesterol, impairing their ability to make vitamin D, and who are afraid of sun exposure.Somehow, the general population has not only been convinced the human immune system was conferred by multiple injections in childhood, but also that one’s own cholesterol is a sinister, dangerous substance. We are a drug-soaked culture. Sixy-six percent of U.S. adults take pharmaceuticals, and half of U.S. seniors take four or more prescription drugs.
The statin drugs sit at the top of this heap. Although I mentioned earlier that the statin industry was worth $10 billion in 2019, it has been projected to rise to $1 trillion per year worldwide, even despite the expiration of their patents. The medical system’s nationwide, multidecade statin-saturation campaign was most likely conducted in the profit-seeking pursuit of Big Pharma’s shareholders’ best financial interests. It would be naïve to deny such an influence over the medical industry.
A newfound appreciation of our immune system and the vital roles of cholesterol and vitamin D in human health may someday eclipse and even reverse our fascination with statin drugs.
Reposted from Colleen Huber’s Substack
Views expressed in this article are the opinions of the author and do not necessarily reflect the views of The Epoch Times. Epoch Health welcomes professional discussion and friendly debate. To submit an opinion piece, please follow these guidelines and submit through our form here.








