

Covid Research Waste - Antivirals: Mega Bin 2
Covid Research Waste - Antivirals: Mega Bin 2
A further 1.2 billion Pounds down the drain


A decade ago, we showed that the UK government wasted over £500 million on stockpiling antivirals for the next “influenza” pandemic. It apparently justified its decision on the basis of the usual models and pharma-sponsored ghost-written trials.
After four years of analysing the data for clinical study reports on antivirals, our Cochrane review reported that while oseltamivir and zanamivir have small, non‐specific effects on reducing the time to alleviation of influenza symptoms, neither drug reduced the risk of developing symptomatic influenza. Treatment trials also did not show a reduction in the complications of influenza (such as pneumonia). They do, however, show neurotoxicity.
Needless to say, The Department of Health considered the UK world-leading in its pandemic preparedness. Britain was recognised as "one of the best-prepared countries in the world for a potential flu pandemic", and "our stockpile of antivirals is a key part of this”.
However. the UK’s propensity to waste money on antivirals seemingly has no limits.
In October 2021, the government purchased 480,000 courses of molnupiravir (made by MSD) and 250,000 courses of the combination of PF-07321332 and ritonavir (Pfizer), neither of which has been approved by the UK’s drug regulator. Two months later, the government signed contracts to secure a further 4.25 million courses.
PF-07321332 and ritonavir, known as Paxlovid, was approved in the UK in December 2021. The UK’s MHRA says it undertook “a rigorous review of its safety, quality and effectiveness.”
The approval reports a trial in high-risk adults with symptomatic covid and reports that five days of Paxlovid reduced covid 19 hospitalisation by 89% at 28 days. Treatment had to be started within three days of the onset of symptoms and was approved for people with mild to moderate covid who are at high risk of developing severe covid.
When the UK was generating large stockpiles of antivirals for the ensuing catastrophe, we pointed out in the Telegraph that “our current approach to interpreting science is too rapid and simplistic. As a consequence, indisputable facts are established overnight. The sheer speed at which data are interpreted generates overconfident, pessimistic predictions about what might happen next. As a result, we seem to be losing the ability to think critically.”

Yes, we were overreacting: the same month, the government signed contracts to secure a further 4.25 million courses, which led to the waste of hundreds of millions of taxpayer money.
By the end of November 2023, over 1.5 million courses of Paxlovid expired unused in European countries, costing nearly €1 billion. The UK saw the greatest loss: roughly 1 million courses expired at a cost of £550 million.
As if this wasn’t enough - next month's forecast estimates that 3.1 million courses will expire in Europe by the end of February 2024, costing €2 billion.
The UK’s gung-ho approach means it bears the brunt of the losses: 550,000 more courses are due to expire by the end of February, and a further 650,000 at the end of June 2024. In total, the UK will have lost nearly £1.2 billion.
Open Prescribing data can help us understand Paxlovid uptake in primary care so far:
It first appeared in the prescribing data in July 2022. Paxlovid’s use increased when NICE issued guidance at the end of March 2023 on COVID-19 antivirals prescribed in primary care for eligible patients. NICE recommended Paxlovid in those at increased risk of progression to severe covid.
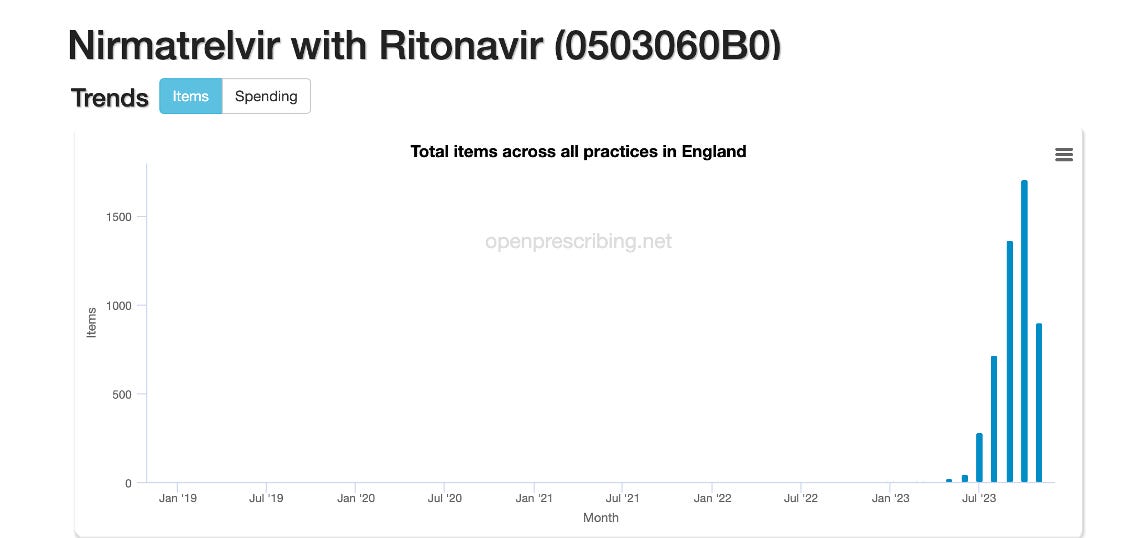
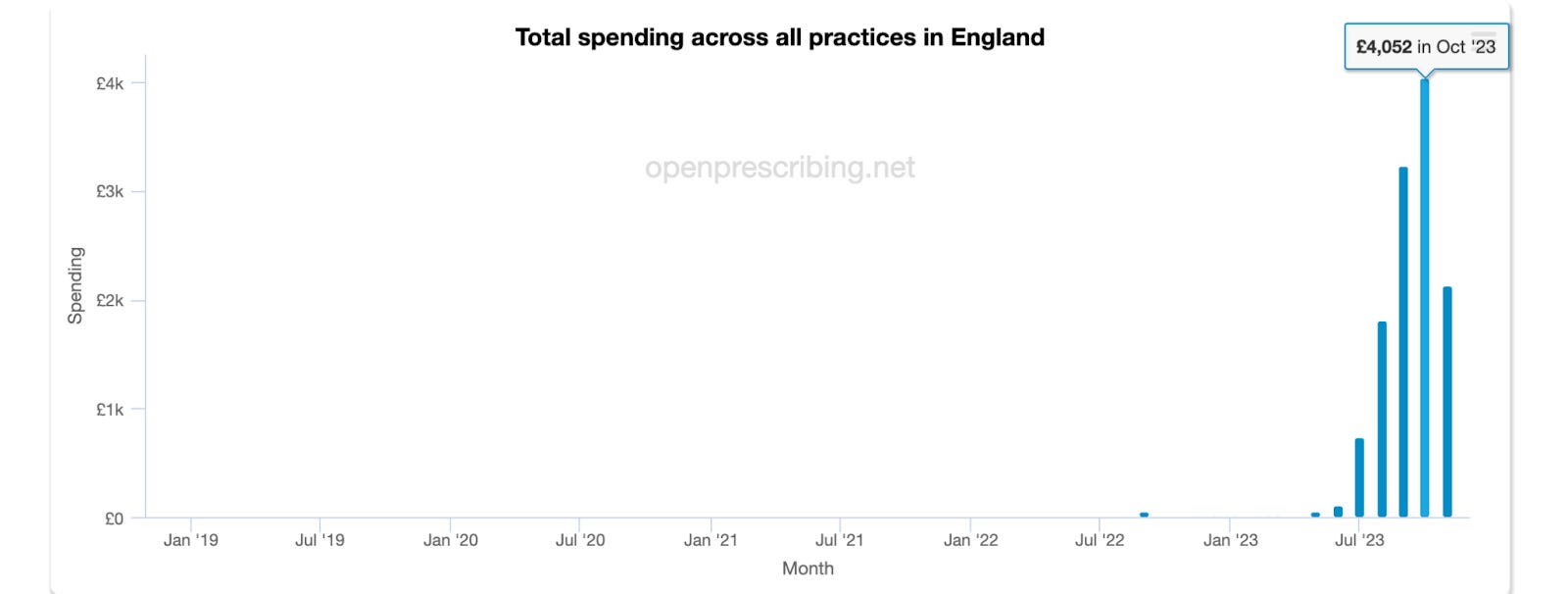
However, the Open Prescribing data so far shows minimal uptake: 5,071 total items have been prescribed across all practices at a cost of £122,000, which peaked in October 2023 at a monthly cost of £4,052.
In its recommendations, NICE also highlighted that “Most of the clinical evidence for these treatments is highly uncertain because it comes from studies done before the dominant Omicron variants of SARS‑CoV‑2 (the virus that causes COVID‑19).”
The rationale for using medicine comes down to clinical medicine and an evidence-based approach, not what politicians think.
The absence of high-quality evidence has resulted in rational GP prescribing, which shows the UK government has failed to learn any lessons over the last decade in terms of stockpiling cost-effective medicines.
We cannot account for the hospital prescribing, but there is no chance that the stok[ile will be used based on current prescribing.
More than half a million courses expire at the end of February, and a further 650,000 will expire by June 2024. Consequently, billions of pounds that could be used more wisely will yet again go to waste - the UK will have lost nearly £1.2 billion in two and half years on stockpiling unused antivirals.
Our experience with government promotion and stockpiling of Tamiflu and Relenza have made us quite wary of extensive promotion and expenditure on antivirals. However, it seems that our work and the warnings of the Council of Europe after what can be loosely called the 2009 influenza pandemic have fallen on deaf ears.
What are we witnessing here?
Amnesia and lack of scientific preparedness by government advisors?
A political “we must be seen to be doing something”?
Corruption at a stratospheric level?
Government subsidies to big pharma?
All four of these?
None of this waste can be ascribed to the precautionary principle - By December 2021, the evidence pointed to less severe outcomes with the Omicron strain; however, the modelling, the overnight experts and the government messaging ensured that vast sums were spent stockpiling huge quantities of a drug that wasn't needed.
In 2014, we identified issues with antiviral stockpiles. However, a decade later, we have made the same mistake. This time, the cost has been more than twice the Tamiflu stockpile. The question now is, how much will it cost to maintain the current stockpile and how much will be needed for the next pandemic?







Covid Research Waste - Antivirals: Mega Bin 2
After the 2009 swine flu scam, how could the Covid debacle happen?
HOW COULD IT HAPPEN?!
The BMJ reported on conflicts of interest etc re swine flu in 2010, see: WHO and the pandemic flu “conspiracies”: https://www.bmj.com/bmj/section-pdf/186584?path=/bmj/340/7759/Feature.full.pdf
And yet the scientific and medical establishment lapped up the batshit crazy, but oh so lucrative Covid response. Critical thinking was AWOL, and self-interest was paramount.
Have any people in ‘the establishment’ any clue about ethics?
How have our parliaments and institutions been so thoroughly corrupted?
An appalling waste. Why stockpile almost useless drugs when you only need to treat the very sick with drugs that work? The very sick are a tiny fraction of those who get infected with SARS-CoV-2 - but part of the existential problem is that lay people (and many doctors) still confuse SARS-CoV-2 infection with Covid-19. You need to treat the latter, not the former.
While I would still insist on steroids/tocilizumab for myself, the ivermectin row continues. Looking at the adverse event profile compared to everything else (including specific antivirals) its pretty safe, so I fail to understand the hysterical reaction against anyone who recommends it. Anyone with any financial sense should be arranging the stockpiling of it.