

Smokescreens - Part 10


One of our readers, Robert Dingwall, drew our attention to a paper called “Making Sense of Mortality” by the late sociologist Lindsay Prior. Dingwall also shared a reading list of related work he compiled some years ago, which is appended to this post.
We cannot reproduce Prior’s work for copyright reasons, but we can summarise his important observations on the process of ICD coding and death attribution.
Working on Northern Irish death certification, Prior kicks off by describing the certificate and conducting a descriptive review of the well-known wide discrepancies between what is written on the certificate and some other source of information such as case notes or post-mortem examinations.
Prior reports the discrepancies between certification and other sources of death information as varying between 93 to 35 per cent, a very variable and wide margin.
He mentions infections as one of the two areas with the widest margins of discrepancies (the other being cerebrovascular disease). He also comments on the higher weight given to social judgement rather than clinical evidence.
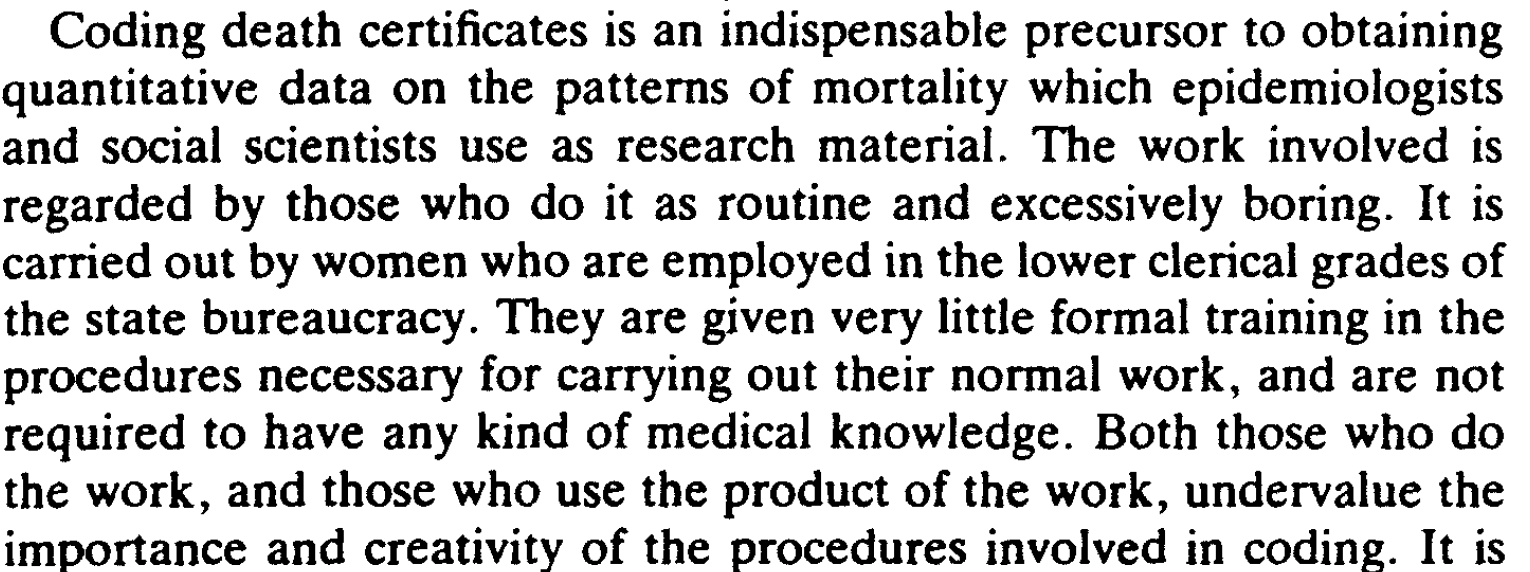
Here is a striking example from Prior’s paper:
Prior then makes the point that too little or too much information may hamper correct adjudication of the cause of death.
He reviewed 10% of 4,150 death certificates filed in 1981 in Belfast and noted that “71.6 percent were found to contain more than one piece of diagnostic information and almost 10 per cent contained four or more items of information, but only one of these items can be selected for coding”. On the opposite side, 28% contained only one piece of information, while 63% contained two to three pieces of information.
This leaves ample scope for the selection of diagnostic information by the certifying physician for whatever reason, potentially undermining the importance of certificates for epidemiological research. However, this is just the first “filter”. Worse is to come.
In the interest of brevity, we will leave aside the issue of the quality of demographic information, which Prior considers essential in correct death adjudication and his review of the 1971 Brodrick Committee’s work on certification of death and focus on the issue of coding of causes of death. At the time, the 9th version of the ICD was in use, a direct descendant of Farr’s, Nightingale’s and Bertillion’s “nosologies”.
Codes are assigned by trained coders following the rules of the manual, but:

And
We do not know who predominantly does the coding. However, it is likely that the work is still regarded as boring and low grade - while knowing why people die is anything but low grade.
The basic principle is assigning what Prior calls “primacy” to a condition as the cause of death. Primacy is the assignment of hierarchical importance, necessary when you have more than one piece of information. Prior lists six types of primacy he observed in the coding of certificates. Again, for the sake of brevity, we will not report them (and the similar problems in coding occupation/social class), but the bottom line is that coders can have a degree of latitude in attribution and death certificates can have limited epidemiological value because of the sheer clinical and social complexity of the synthesis of very small or huge amounts of information and their placement in a hierarchical order.
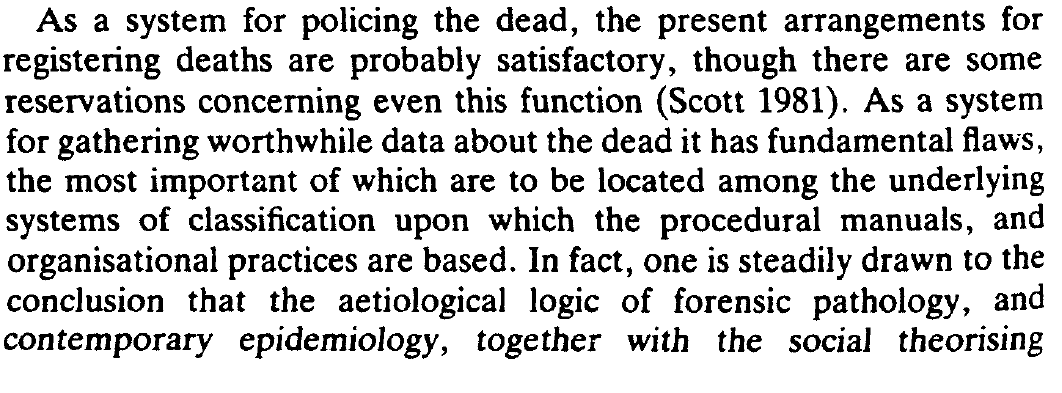
Here are some of Prior’s conclusions - note that he was writing before the Shipman case exposed systemic weaknesses in UK registration processes:

The Office of Population Censuses and Surveys (OPCS) is the predecessor to the ONS. Although much of the process is now automated, this has not eliminated the fundamental problems identified by Prior. The algorithms encoded in the software still embody the results of human decisions about organising and classifying the raw data on death certificates.
Prior’s insights and conclusions are supported by the papers in Dingwall’s list and other studies looking at discrepancies between entries on death certificates and post-mortem diagnoses. For example, one series of 433 autopsies from Iceland by Nielsen et al. found around 50% overall disagreement and around 25% disagreement on the cause of death after the post-mortem examination.
Prior’s work is powerful and insightful in explaining all the contradictions and inconsistencies discussed in this series. It is social science at its very best. We recommend you read the paper. Good work such as Prior’s is immortal, so ignore the 1985 label.
Readings
Prior L. Making sense of mortality. Sociol Health Illn. 1985 Jul;7(2):167-90. doi: 10.1111/1467-9566.ep10949063.
Nielsen GP et al. The accuracy of death certificates. Implications for health statistics. Virchows Arch A Pathol Anat Histopathol. 1991;419(2):143-6. doi: 10.1007/BF01600228.
Selected bibliography on the social construction of official statistics.
Atkinson, J. Maxwell. 1978. Discovering Suicide: Studies in the Social Organization of Sudden Death. London: Macmillan.
Bloor, Michael J. 1991. A Minor Office: The Variable and Socially Constructed Character of Death Certification in a Scottish City. Journal of Health and Social Behavior, 32, 273-287.
Churchill, L. (1971). Ethnomethodology and measurement. Social Forces, 50, 182-191.
Cicourel, Aaron V. 1964. Method and Measurement in Sociology. New York: Free Press.
Espeland, Wendy and Mitchell Stevens, “A Sociology of Quantification,” European Journal of Sociology (Archives Européennes de Sociologie), 49(3):401-436, 2009.
Garfinkel, Harold. 1967. Studies in Ethnomethodology. Englewood Cliffs, NJ: Prentice Hall.
Hindess, Barry. 1973. The Use of Official Statistics in Sociology. London: Macmillan.
Kitsuse, J., and Cicourel, A.V. (1963). A note on the uses of official statistics. Social Problems, 11, 131-139.
Subscribe to Trust the Evidence
Informing health decisions by separating evidence from opinion







Smokescreens - Part 10
In the 1980's autopsies formed a regular part of my work to determine the cause of death of patients who had been treated for haematological malignancies and those who had received a stem cell transplant. We needed to distinguish between death due to an intercurrent infection and that which resulted from refractory or recurrent haematological disease. Often times infection concurred with active haematological disease. Unfortunately, since then , the number of autopsies done has declined to the extent that they are sas rare as hen's teeth these days. Quite apart from anything else this makes accurately attributing the cause of death well nigh impossible so most entries in the death certificate are bound to be subjective. Moreover , the entry is also dependent on who completes the certificate. For instance, when a patient dies with refractory leukaemia and has also developed pulmonary aspergillosis, a haematologist would rather emphasise the infection whereas a microbiologist would rather focus on the haematological disease. COVID-19 is associated with so many non-specific symptoms that attributing cause of death without the help of a reliable diagnostic test just can't be done. If governments were really that keen on finding the facts they would have insisted that the medical profession attempted to investigate deaths and code them properly. Indeed they could have also required the vaccine producers to fund autopsies and appropriate postmortem investigations on every 10th patient who died affect receiving a vaccine injection. The lack of interest around mortality is enough to make a scientist weep!
Hi Will, thanks for the comment. I think (think, not have evidence in hand) that it is perfectly plausible that SARS-CoV-2 was knocking around somewhere in a number of deaths but I cannot answer on the sequence of events nor the %. As you know we found 14 different definitions of death by or with Covid so your guess is as good as mine.
Helen describes the subjectivity of some diagnoses beautifully.
There is also the problem of the abuse/misuse of PCR which we will cover in the Riddles series if we run it again.
Best wishes, Tom.