

Smokescreens - Part 4
Smokescreens - Part 4
Death yes, by: well, maybe, perhaps….


In our fourth post, we will try and answer the questions on the attribution of deaths:
“How do you decide that someone died of the F word and not, say, of a myocardial infarction or infection with Mycoplasma Pneumoniae (not a virus, but an equally nasty customer)?
If the F word plays a role in a death, how exactly do you attribute that role?
Is it the F word that kicks off the sequence of events leading to a demise, or does the F word play a relatively minor role? Is it a bystander?”
The central question in this case is how causes of death are recorded and attributed.
In England and Wales, the current Medical Certificate of Cause of Death (MCCD) is set out in two parts:
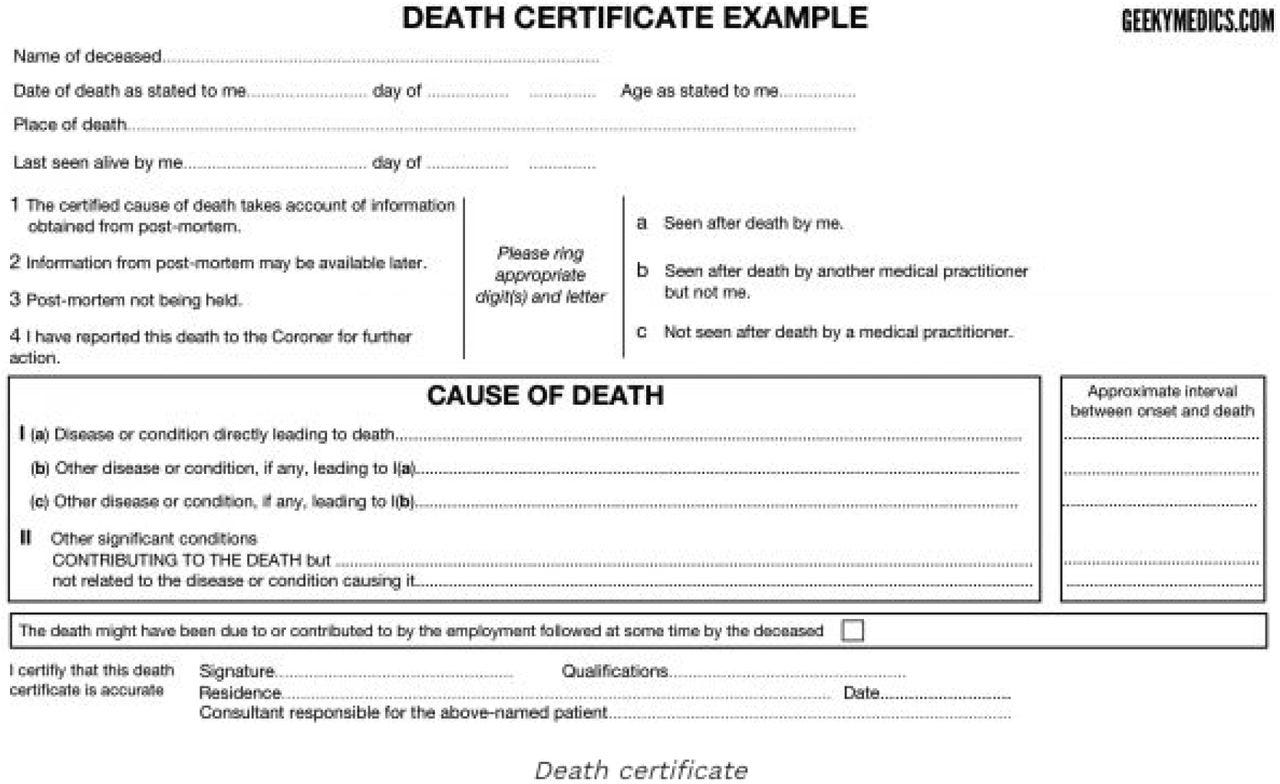
Part 1. The immediate, direct cause of death is reported on the certificate. The medical practitioner should go back through the sequence of events or conditions that led to death on subsequent lines until reaching the one that started the fatal sequence. The condition on the lowest completed line of part I will have caused all of the conditions on the lines above it. This initiating condition, on the lowest line of part I will usually be selected as the underlying cause of death, following the ICD coding rules. The WHO defines the underlying cause of death as “a) the disease or injury which initiated the train of morbid events leading directly to death, or b) the circumstances of the accident or violence which produced the fatal injury”. From a public health point of view, preventing this first disease or injury will result in the greatest health gain.
Part 2. Other diseases, conditions, or events that contributed to the death, but were not part of the direct sequence, are recorded in part two of the certificate. The conditions mentioned in part two must be known or suspected to have contributed to the death, not merely be other conditions that were present at the time.’
On the basis of the content of the death certificate, trained coders (not medical practitioners) assign the ICD code, with each death as a block contributing to the running total. However, the adjudication process is carried out in the absence of notes, pm reports or any other evidence.
So, what the practitioner writes on the certificate is what gets coded. It is rare for any viral respiratory disease to lead directly to death. The most likely subjects of the death certificate are elderly people with multiple pre-existing conditions. Deciding what comes first, second and third and the role played by each is decidedly difficult.
In our fictitious patient B if there is an initial verified influenza episode directly leading to pneumonia and respiratory failure, it is a very reasonable assumption that influenza is the underlying cause of pneumonia with respiratory failure and death.
However, if influenza is a laboratory finding in multi-system failure (kidney, respiratory, cardiovascular, for example), how should we decide what role it plays? What if there is more than one agent present?
These grey areas may be clarified by the Medical examiners - independent review (see final draft regulations) of all non-coronial deaths from April 2024. Briefly, “there will be an independent review of all deaths in England and Wales, without exception. This will either be provided by independent scrutiny by a medical examiner or by investigation by a coroner”. A new MCCD will add a line (1d on the cause of death) and include information on the ethnicity of the deceased (where available) and whether the deceased was pregnant or recently pregnant.
The details on the new rules regarding the MCCD are here.
We could not find any specific mention of investigating the sequence of events, but the additional information may prove important, as well as the recognition that the current system is vague and prone to errors.
Of note is that the rationale for introducing a statutory requirement is reported as “.....learning from the COVID-19 pandemic”, although what the DHSC has learned is unclear, and the text only refers to including additional information about the deceased ethnic group.
So, attribution of death causes is an imprecise science unless you have a situation like massive trauma. It is probabilistic and not certain.







Smokescreens - Part 4
My impression was,during covid, no practitioner examined the deceased. If true then this would make inaccuracy the norm particularly where death occurred outwith a hospital setting.
There is a classic medical sociology paper on the coding process by the, sadly missed, Lindsay Prior. This was based on direct observation in the Belfast Registry Office. Published in 1995, some institutional and legal details may have changed but the challenges probably haven't
https://doi.org/10.1111/1467-9566.ep10949063