

The predictable, unpredictability of respiratory pathogens
The predictable, unpredictability of respiratory pathogens
What surveillance tells us about seasonal respiratory illnesses


Winter is entrenching itself in the Northern Hemisphere, and as we approach the equinox, the predictable respiratory pathogens are taking hold.
The National Influenza and COVID-19 report monitors seasonal respiratory illnesses. The latest report summarises surveillance systems in England from week 43 (between 23 and 29 October 2023).

SARS-CoV-2 positivity decreased to 8.7% compared to 9.7% in the previous week.
Positivity for RSV is on the increase at 8.7%,
RSV usually causes mild, cold-like symptoms, but it can be serious, particularly in infants and older adults. It is worth noting the highest RSV positivity was seen in those aged under five years old at 34%.
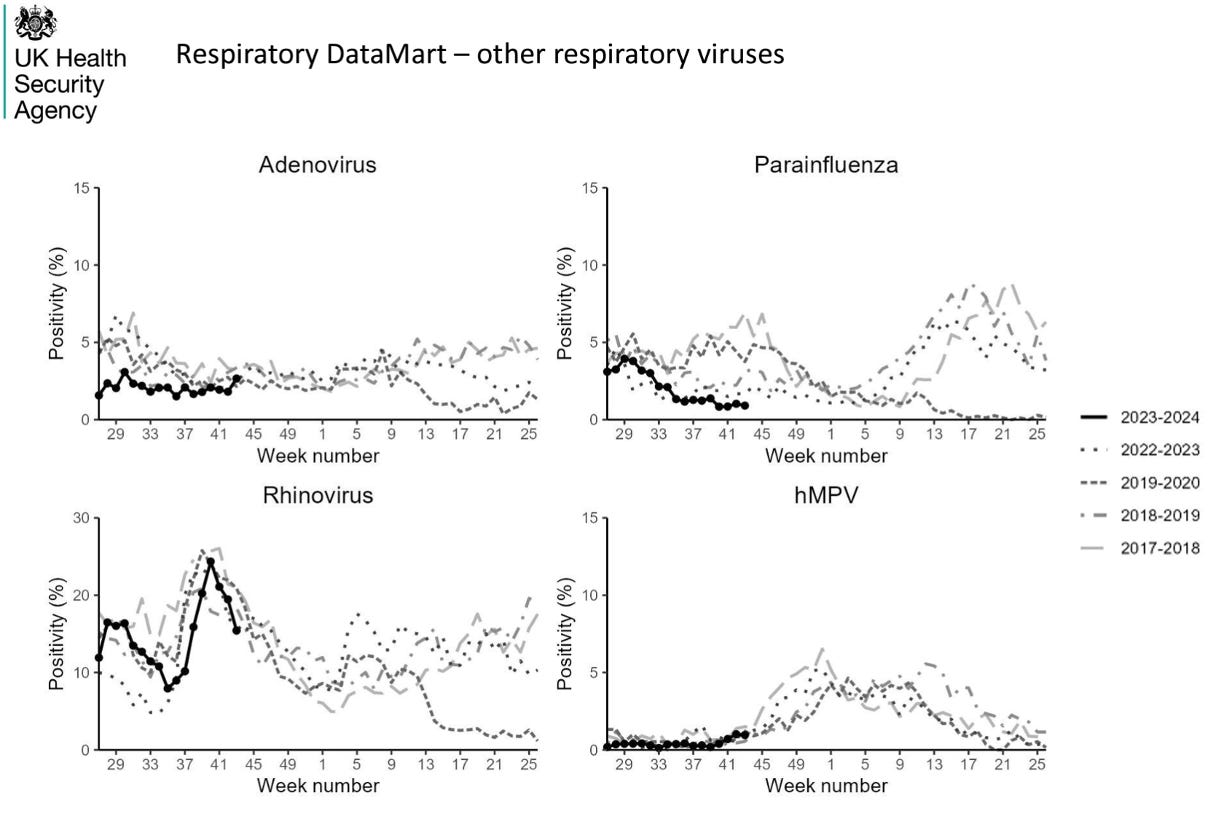
Rhinovirus - which seems to stick around whatever - positivity decreased to 15%, with the highest positivity seen in children under five years old at 25%.
While rhinovirus is the most common cause of the common cold, it can cause severe disease in those with a weakened immune system.
Primary care surveillance reports influenza-like-illness (ILI) consultations decreased slightly to 3.2 per 100,00. This slight decrease is likely due to the half-term school break; expect a rebound from here on in.
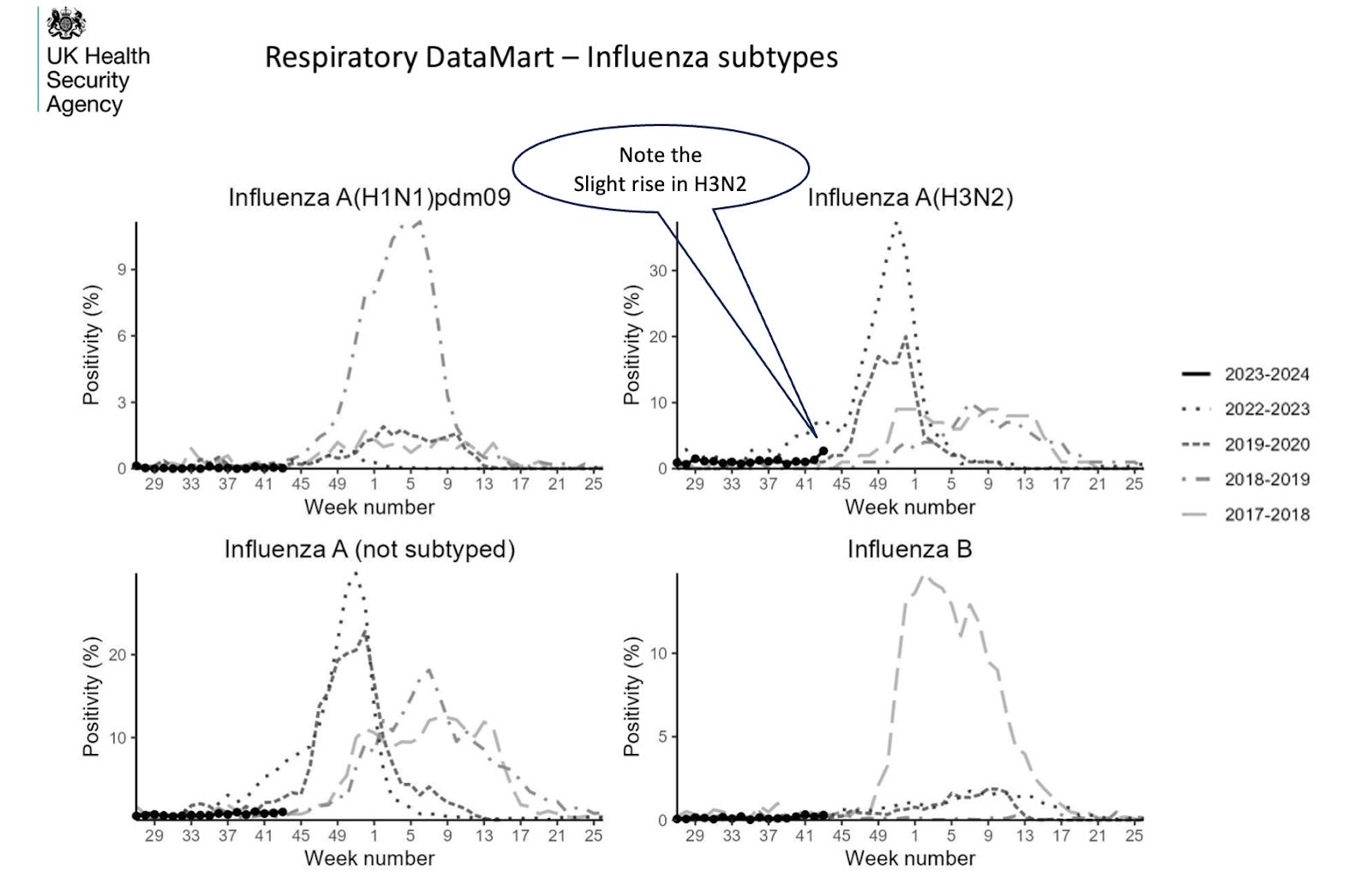
Influenza positivity remained stable, hovering around 1.3%. However, note the slight rise in H3N2, which was the cause of the 1968 pandemic. Since then, H3N2 has genetically and antigenically evolved to contribute to many seasonal epidemics and can be associated with more severe influenza seasons.
Last winter, the Health Secretary, Steve Barclay, blamed “flu and COVID for the NHS crisis as pressure mounted on the government to act. In addition to the Scarlet fever scare, Barclay considered “massive pressures" led to the winter crises. Steve seemed not to be aware of the predictable rise in infections that occur each year. Health leaders said "structural problems" need to be addressed, but little has changed for this winter preparedness.
We’ve previously pointed out that ‘it doesn’t take much to work out that you’ll quickly run into trouble with the slightest increase in daily admissions, ’ what is also predictable is the predictable response to the winter crises. Yet, in 2022, the Coffey plan added nothing to capacity.
But all is not lost: NHS England's two-year delivery plan for recovering urgent and emergency services includes a promise of 5,000 new beds and 800 new ambulances, which will apparently be on the road by this winter. However, the BBC reports the promises don’t add up - most of the vehicles being ordered by trusts are replacements.
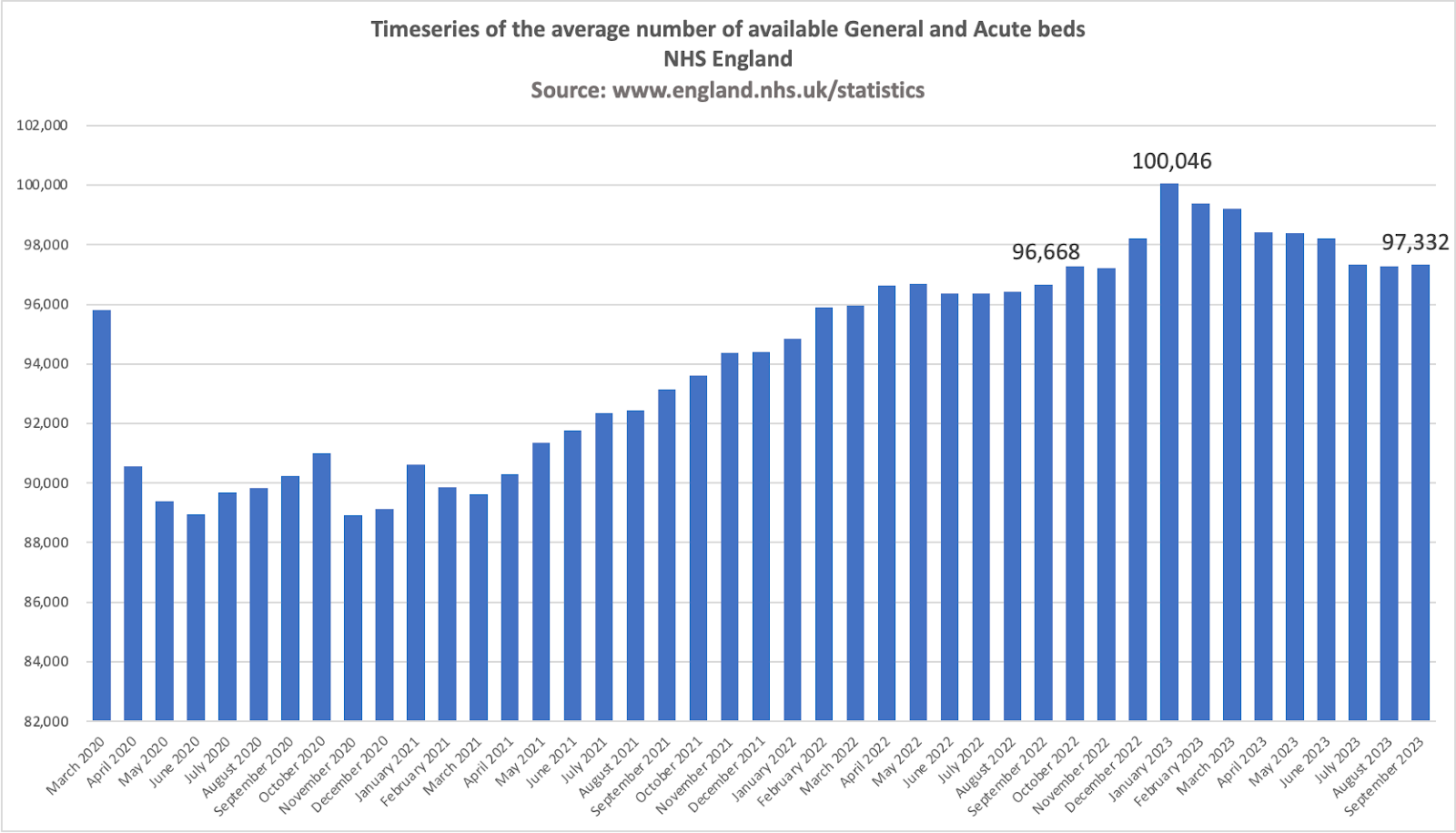
Also, we’re left wondering where all these beds will come from: NHS England’s Statistics on Bed Availability and Occupancy report for this September, there are 97,332 general and acute beds, up by 664 from this time last year. Bed numbers peaked in January at 100,046, so if the promise is to be realised, then some 7,700 beds need to be made available.
So, if you can't be ready for each winter’s pressures, how can you expect to be prepared for a pandemic? Maybe a question for the Inquiry.
Also, when anyone tells you, “the flu” is on the rise, I have the “flu”, or “flu is the cause of the crisis, " then they are referring to all those agents that are contributing to influenza-like illness. Telling one of these agents from the other based on symptoms alone is difficult, given they all can cause fever, sore throat, coughing, nasal discharge, headache, and muscle pain.
As you can see, these agents are endemic, continuously circulating to a greater or lesser degree. What’s unpredictable is which agents and which variants will contribute most to the mix this winter and the exact date they’ll take off and inevitably hit the media when the crises has arrived.







The predictable, unpredictability of respiratory pathogens
The closure of smaller ,local hospitals often known as cottage hospitals , causes inappropriate use of expensive acute beds. Many ,particularly elderly , patients with severe respiratory problems need extra care not intensive care. Plus in my case the nearest hospital is 6 miles away ,or two buses each way , making visiting more difficult for friends and family. So some of the capacity could be increased at a lower cost and if more local lower ambulance transport mileage costs .
I am not saying more capacity is not needed, but I am also wondering if there is a fundamental problem with protocolised, rather than individualised medicine?
Diagnostic test being done as this is the next test on the protocol, rather than taking a more holistic approach? This leads to unnecessary tests, unnecessary costs and time-delays waiting for these tests to be done and results to be interpreted.
Just asking.