

 PDF
PDFAbstract
The SARS-CoV-2 outbreak has disrupted the delivery of routine healthcare services on a global scale. With many regions suspending the provision of non-essential healthcare services, there is a risk that patients with common treatable illnesses do not receive prompt treatment, leading to more serious and complex presentations at a later date. Lemierre’s syndrome is a potentially life-threatening and under-recognised sequela of an oropharyngeal or dental infection. It is characterised by septic embolisation of the gram-negative bacillus Fusobacterium necrophorum to a variety of different organs, most commonly to the lungs. Thrombophlebitis of the internal jugular vein is frequently identified. We describe an atypical case of Lemierre’s syndrome involving the brain, liver and lungs following a dental infection in a young male who delayed seeking dental or medical attention due to a lack of routine services and concerns about the SARS-CoV-2 outbreak.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com

Background
Fusobacterium necrophorum is an anaerobic gram-negative rod. Though commonly found in the oropharyngeal flora of healthy individuals, it has potential to cause severe localised and disseminated infection, including the eponymous ‘Lemierre’s syndrome’.1 Though no strict definition of Lemierre’s syndrome is agreed on, most publications agree it includes a recent oropharyngeal infection, clinical or radiological evidence of internal jugular vein (IJV) thrombosis and isolation of an anaerobic pathogen (mainly F. necrophorum).
Population-based studies suggest that F. necrophorum most commonly affects young, otherwise healthy individuals.1 2 The median age of onset is 19–22 years affecting two times as many males as females.
Described as ‘life-threatening but curable’, Lemierre’s syndrome has a mortality rate of 4%–12%.2 Reported incidence of Lemierre’s syndrome has increased in recent years.2–4 The increasing incidence of this previously ‘forgotten’ disease is thought to be due to antimicrobial stewardship efforts resulting in decreased antibiotic prescribing for upper respiratory tract infections,3 while improving laboratory techniques may also be contributing to an increased detection rate.4
With many countries imposing travel warnings, restrictions of movement and lockdowns during the SARS-CoV-2 pandemic, emerging data suggest a delay in patients seeking care for urgent conditions.5 Furthermore, postponement of routine outpatient visits and elective procedures risks delaying diagnostic and therapeutic interventions, with severe impact on patients’ health.6
At a time when the SARS-CoV-2 outbreak has disrupted the provision of routine healthcare services on a national and global scale, we describe a delayed presentation of disseminated F. necrophorum infection in an immunocompetent young male, in a case that emphasises the importance of encouraging patients to seek urgent medical care during a pandemic.
Case presentation
A 24-year-old man presented to the emergency department during the outbreak of the SARS-CoV-2 pandemic. He reported a 3-week history of headache, myalgia, left lower limb weakness, abdominal pain and anorexia. He also described shortness of breath, unstable gait (requiring assistance to walk) and right elbow pain. Three weeks prior to presentation, he had experienced periodontal swelling and tenderness, which he described as a ‘dental abscess’. He had not sought dental services at this time, and had subsequently delayed seeking medical attention, citing concerns about attending hospital due to the risk of contracting SARS-CoV-2.
He had no medical history of note, but had undergone extensive dental procedures as a teenager (fillings to lower molars and dental extraction). He was heterosexual with no history of high-risk sexual activity and had no history of intravenous drug misuse.
On examination, he was tachypnoeic, tachycardic, normotensive and afebrile. Oxygen saturations were well-maintained on room air. Examination of the thorax revealed right basal crepitations with no cardiac murmurs. Neurological examination revealed left lower limb weakness and dysarthric speech. The abdomen was tense with no focal tenderness. The right elbow was markedly swollen and tender, with reduced range of movement. Oral examination revealed marked tooth decay of the left lower molars, with no tonsillar enlargement or pharyngitis. No neck swelling or tenderness was reported.
Investigations
Laboratory investigations revealed a microcytic anaemia (haemoglobin 99 g/L), thrombocytopenia (104×109/L) and normal white cell count with lymphopenia (0.5×109/L). Liver function tests were markedly deranged (aspartate transaminase 120 IU/L, alanine transaminase 103 IU/L and bilirubin 37 µmol/L) with hypoalbuminaemia (25 g/L). Inflammatory markers including C-reactive protein (194 mg/L), ferritin (979 µg/L) and D-dimer (1987 ng/mL) were markedly elevated.
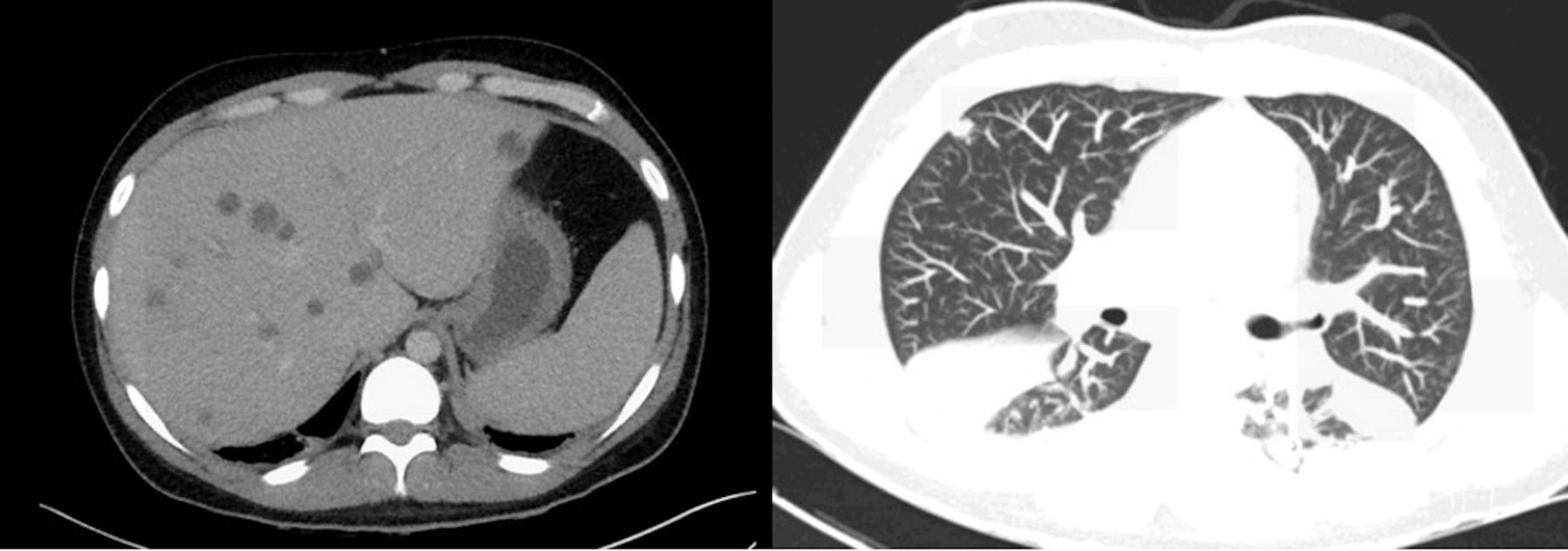
CT of the thorax, abdomen and pelvis revealed multifocal hepatic lesions consistent with disseminated hepatic abscesses and multiple foci throughout the lungs in keeping with septic emboli (figure 1).

CT images demonstrating multifocal hepatic lesions and dense airspace opacifications.
CT of the brain demonstrated multiple foci of hypoattenuation in the brain parenchyma suspicious for cerebral abscesses (figure 2).

CT imaging of the brain demonstrating foci of hypoattenuation in the brain parenchyma.
Transthoracic echocardiogram (TTE) showed no vegetation but a patent foramen ovale was noted. SARS-CoV-2 swab and blood-borne viral screening were negative, while MRI of the brain demonstrated multifocal abscesses in both cerebral hemispheres (figure 3). Initial CT angiogram of the neck revealed bilateral dental abscesses but no neck collection or abscess, and no filling defect within the vasculature. However, a subsequent CT angiogram during the course of the admission revealed a filling defect within the left internal jugular vein (figure 4). No further filling defects were identified within the surrounding vasculature, including the lingual and tonsillar veins.

MRI image revealing multifocal abscesses in both cerebral hemispheres.

CT angiogram images demonstrating a filling defect within the left internal jugular vein.
A transesophageal echocardiogram was not performed given the unremarkable TTE and confirmation of an alternative source of infection, coupled with hospital-wide efforts to limit aerosolising procedures during the SARS-CoV-2 pandemic.
Differential diagnosis
At the time of admission under the general medical team, differentials under consideration included infective endocarditis, SARS-CoV-2 infection with superimposed bacteraemia and HIV with an associated opportunistic infection.
The possibility of a disseminated sexually transmitted infection, septic arthritis or an underlying malignancy was also considered.
Treatment
Intravenous antibiotics including ceftriaxone, vancomycin and metronidazole were commenced following collection of three sets of blood cultures. Intravenous fluids were administered.
Consultation was sought from orthopaedic and maxillofacial surgical teams, as well as infectious disease, cardiology and haematology specialists.
Within 24 hours, a gram-negative bacillus was confirmed in the anaerobic blood culture bottle, subsequently identified as F. necrophorum.
On day 2 of admission, our patient was transferred to the intensive care unit (ICU) for surveillance. On day 4, his clinical status deteriorated, developing type one respiratory failure and requiring intubation. He remained intubated for 18 days, during which the time he underwent interventional radiology guided drainage of liver abscesses and dental extraction of two retained dental roots and six decayed teeth on both sides of the mouth.
Therapeutic dose enoxaparin was initiated following detection of the filling defect within the left internal jugular vein, before switching to apixaban prior to discharge.
Outcome and follow-up
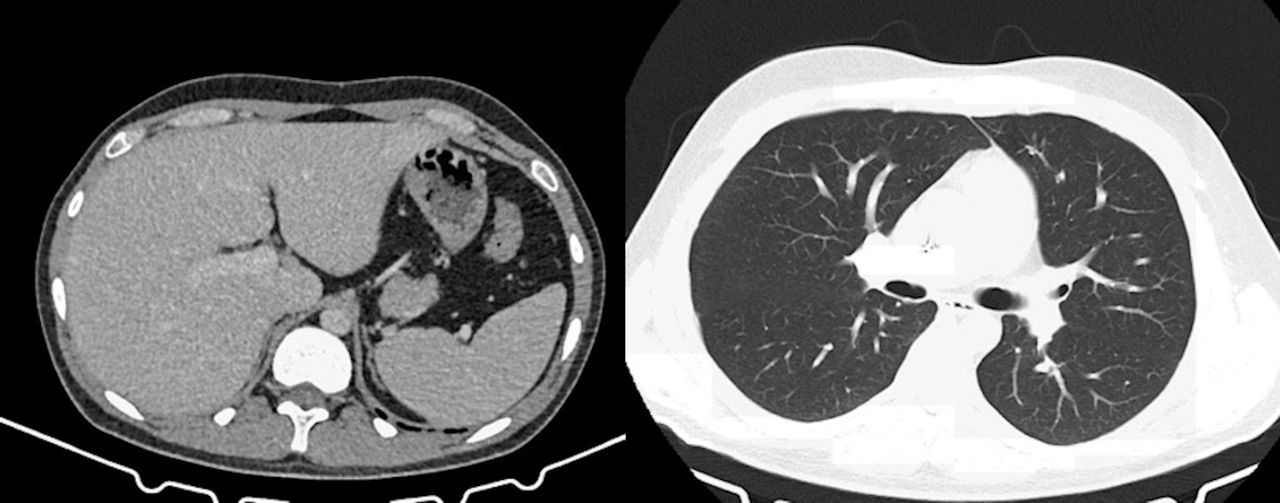
After 3 weeks in ICU and a further 2 weeks of ward-based rehabilitation as an inpatient, our patient was afebrile, symptom-free and mobilising with one crutch. Repeat imaging demonstrated marked improvement in the hepatic abscesses. He was discharged home to continue intravenous ceftriaxone and oral metronidazole via the outpatient parenteral antimicrobial programme, with plans to continue his anticoagulant therapy for 3 months. Follow-up was arranged through the infectious disease clinic and repeat imaging at a 4-week interval showed resolution of hepatic abscesses, resolution of pleural effusions and airspace opacifications (figure 5), with considerable reduction in intracranial abscesses.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Repeat CT imaging demonstrates resolution of hepatic abscesses, pleural effusions and airspace opacifications.
Discussion
Currently, there is no universally accepted definition of Lemierre’s syndrome. One Danish epidemiological study defined it as a septic case of F. necrophorum infection (confirmed in blood cultures), with a primary focus in the head and neck (typically of oropharyngeal origin), disseminated to nearby or remote regions.2 Some authors specify that the infection must originate in the throat (thus excluding infections arising from the ears, teeth or mastoid region), while others do not require isolation of F. necrophorum to confirm the disease.4
The complexity of the disease and the variable clinical presentation makes a concise definition difficult. As such, it is essential that clinicians across the myriad specialties recognise the wide range of signs and symptoms that should raise suspicion of Lemierre’s disease.
While the majority of cases are of oropharyngeal origin, Lemierre’s syndrome can also arise as a complication of an odontogenic infection,7 and disseminated F. necrophorum infection has even been described following routine dental cleaning.8
Cases of metastatic spread of F. necrophorum involving the lungs, liver, meninges, endocardium, skin/soft tissue, bone, joints and even the peripancreatic tissues have all been described.2 4 9 Renal and cerebral abscess have also been reported, but are rare.3
While the majority of cases feature pulmonary involvement, our case is unusual in that our patient presented with signs and symptoms resulting from widespread embolisation across a multitude of different organs. Furthermore, brain abscesses are thought to result from retrograde intracranial extension of IJV thrombosis.3 In our case, CT imaging identified intracranial abscess formation prior to the detection of IJV involvement, suggesting an alternative route of seeding—perhaps via the patent foramen ovale (though allowing for the possibility that IJV involvement was simply not visible on the initial CT).
We also acknowledge that the non-occlusive lesion observed in the IJV on repeat CT imaging of the neck could have represented thrombosis secondary to recent catheterisation.
Recommended treatment typically involves antimicrobial therapy with a beta-lactam agent and metronidazole for 3–6 weeks.3 Where accessible, drainage of abscesses is also advised.4
Though some articles describe respiratory failure requiring ventilation as uncommon,4 other studies and case reports recommend involvement of the critical care team at an early stage to ensure adequate monitoring and support, with one study reporting intubation in up to 37% of cases.10
The role for anticoagulation in Lemierre’s syndrome remains unclear.11 While anecdotal reports suggest a reduced risk of septic embolic events arising from the IJV thrombosis with anticoagulation,3 other studies suggest that anticoagulation be reserved for patients with retrograde progression of thrombus, as most do well without.4 In our case, given the temporal association between the IJV thrombosis and recent insertion of an intravascular catheter device, a 3-month period of anticoagulation was deemed appropriate. There was no evidence of further embolisation or seeding of infection following initiation of anticoagulation in this instance.
Circumstances surrounding this case—namely the global SARS-CoV-2 pandemic—were intrinsically linked to the course of events. The Irish Dental Association warned that in many places, emergency care could not be provided during the SARS-CoV-2 pandemic due to unavailable or unaffordable personal protective equipment.12 Furthermore, the national restrictions requiring that people stay at home wherever possible may have delayed certain people who might otherwise have sought prompt medical attention.
We describe a severe case of Lemierre’s syndrome, requiring ICU admission and intubation, where presentation and initiation of treatment were delayed by the SARS-CoV-2 pandemic. Our case is unusual in having spread from a periodontal infection, involving multiple organs, and featuring intracranial involvement, initially in the absence of radiological evidence of IJV thrombosis. This could represent intracranial seeding of septic emboli via a patent foramen ovale. Initiation of anticoagulation did not result in detectable increase in embolic events, and a good clinical response was achieved with antimicrobial therapy, abscess drainage and source control.
Learning points
This case highlights the importance of providing medical and dental services during a public health emergency or pandemic; failure to do so may result in hospital admissions with severe illnesses that might otherwise have been treatable in an outpatient setting.
Lemierre’s syndrome can give rise to septic emboli involving multiple sites throughout the body, and should be considered in cases of disseminated infection of unknown origin.
This case demonstrates the importance of considering Lemierre’s syndrome arising from periodontal infection, and how source control should be considered along with antimicrobial therapy and drainage of accessible collections.
Intracranial involvement should be considered and investigated in Lemierre’s syndrome, even in the absence of confirmed internal jugular vein thrombosis.
Acknowledgments
The authors thank Dr Susan Clarke, Consultant Infectious Disease Specialist in St James’s Hospital, Dublin.
References
Footnotes
Contributors FH and LO composed the original draft, with FH taking the lead on the literature review, and LO compiling the case report. FH was also involved in the care of the patient during the course of their admission. NM reported on and compiled the images, reviewed the manuscript and provided critical feedback and advice with reference to the manuscript. RO was the overall supervisor of the project. She helped direct the content and structure of the manuscript, with input into the concept. RO provided critical feedback, and was also the consultant in charge of the care of the patient in question. All authors contributed to the editing and finalising of this manuscript. All authors have given final approval to the version herein attached, and agree to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Request Permissions
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.