Despite the fact that excess body fat contributes to the risk of a number of common diseases, many observational studies have reported that people in the overweight or even obese categories sometimes experience better health outcomes than lean people. This is the "obesity paradox". I covered this concept in detail earlier this year (1).
Yet as with all observational methods, these findings are vulnerable to confounding-- and it can sometimes be profoundly misleading. There are reasons to believe that confounding could be particularly relevant here. First, people who are sick tend to lose weight, making leanness look more dangerous than it really is. Second, cigarette smokers tend to be leaner than nonsmokers, and also much less healthy, also making leanness look dangerous.
Fortunately, there are ways to correct for these potential confounding factors, at least to some degree. The research of Andrew Stokes has shown that when we do so, the obesity paradox goes away (1). Two new studies strongly confirm that when confounding is minimized, there is no paradox.
Study #1: "BMI and all cause mortality: systematic review and non-linear dose-response meta-analysis of 230 cohort studies with 3.74 million deaths among 30.3 million participants"
This is a huge meta-analysis which, as the title suggests, includes mortality statistics from a whopping 30.3 million people of all weights (2).
The thing I really like about this study is that they analyzed several subsets of the data, each of which was progressively less likely to be confounded. If we hypothesize that the obesity paradox is an illusion that results from confounding, then each additional step toward minimizing confounding should make the paradox less apparent.
And that's exactly what happened. In all subjects, as well as current smokers, the lowest mortality level occurred at a body mass index (BMI) of 25, which is on the cusp of overweight. Yet among people who have never smoked, the optimal BMI was 23-24. Among people who had never smoked and who were healthy at baseline, the optimal BMI was 22-23. And among people who had never smoked and were followed up for at least 20 years, the optimal BMI was 20-22! That is quite lean.
The last analysis is a particularly powerful way of avoiding confounding due to existing illness. If you're recording a person's weight right now and their risk of death in 20 years, it's likely that whatever kills them in 20 years is not impacting their weight right now. So you get a cleaner assessment of the impact of BMI on health. This assessment shows that it's much more dangerous to be obese than to be underweight. You can see that in this graph of BMI vs. mortality from the paper:
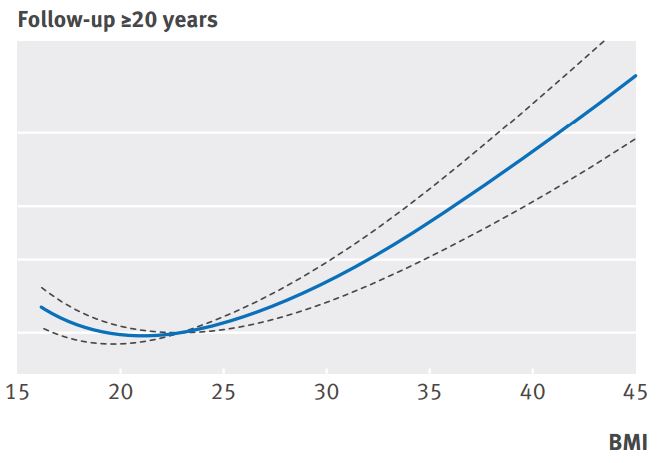 |
| From figure 3. BMI is on the horizontal axis, and mortality rate is on the vertical axis. The horizontal white lines represent relative risk of 1, 1.5, 2, and 3. The top of the graph represents a relative risk of 5. |
Study #2: "Body-Mass Index in 2.3 Million Adolescents and Cardiovascular Death in Adulthood"
This is an Israeli study that, again as the title suggests, measured BMI in 2.3 million adolescents and subsequent death rates in adulthood, with a particular focus on cardiovascular deaths (3).
Like the previous study, this one is remarkable due to the extra-long follow-up period between BMI measurement and death: up to 44 years, with a mean of around 25 years! This means that there was usually a long period of time between the BMI measurement and the death outcome. This is compounded by the fact that the researchers measured BMI in adolescents 16-19 years of age-- a time at which very few people suffer from overt disease. Both of these factors minimize confounding.
When we consider total mortality, remarkably the healthiest BMI range was between 19.7 and 21.4 in men, and between 19.2 and 21.0 in women. That is very lean, but keep in mind that it was measured in 16-19 year-olds, who tend to have a naturally lower BMI. That range was also optimal or nearly so for most types of death reported, including stroke, sudden death, total cardiovascular deaths, and non-cardiovascular deaths. The one exception was coronary heart disease death, which was lowest at the lowest BMI (12-18! Not recommended).
This graph clearly illustrates the consistent relationship between adolescent BMI and later cardiovascular mortality in this study:
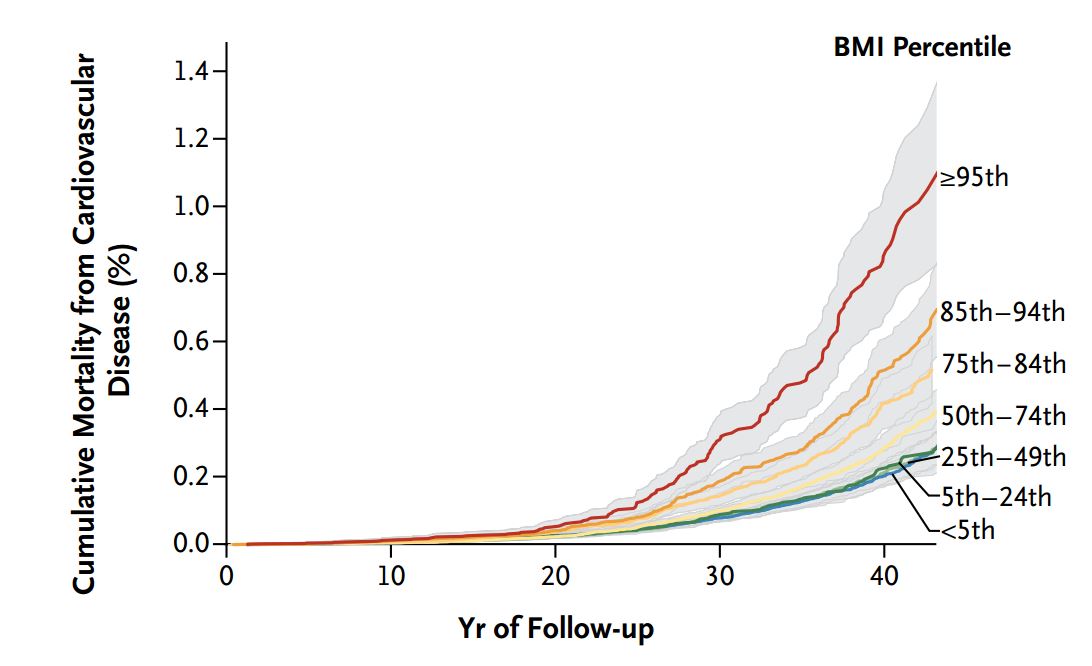 |
| On the vertical axis, we have cardiovascular mortality, and on the horizontal axis, the number of years since BMI was measured. Each line on the graph represents a different BMI category. BMI is listed by percentile rather than absolute values. Lower percentiles represent lower BMIs. |
The longer the follow-up, the more apparent the BMI effect became. Note that at the longest follow-up, cardiovascular mortality risk differed by nearly 4-fold between BMI extremes. This is a huge effect. Again, the risk is concentrated in the higher BMI categories.
Conclusion
Two huge new studies with compelling designs add substantial weight to the hypothesis that there is no obesity paradox. As suggested by controlled studies in animals and humans, excess body fatness likely contributes to chronic disease risk and the overall risk of dying. Risk increases in parallel with excess fat, yet BMI values at the upper end of the lean range, and even into the lower overweight range, don't appear to be especially dangerous (particularly among people with higher lean mass)*. Furthermore, healthy behaviors such as physical activity and a high-quality diet can attenuate risk in people of all weights.
* People of Asian/Indian ancestry may be an exception. Their risk level increases more sharply at a lower BMI level.
14 comments:
Well that's pretty compelling evidence. I guess the conclusion is pretty obvious, I need to grow 6 more inches
As a mortician who specializes in obesity embalming, I can only see the paradox as some form of obesity apologist driven agenda.
It was in no was based on the real world I live in.
I feel like I should now be predicting my future health based on what my weight was back when I was 19, which is unchangeable...
Muscle mass can confound BMI. Not sure that is the whole story, but good muscle mass tends to help BG control - which is associated with cancer and many other life shortening events.
Having 'ideal body fat' might also leave one with less reserves to survive major health events. Quite possible to lose not only fat - but large amounts of muscle during a hospital stay. What if you are low on both?
There is a paradigm shift occurring. The CAD(coronary Artery Disease) narrative is/has-been clearly in need of correction - This Review sort of points out the elephant in the room. Time to bury the cholesterol theory.. One they put the false narrative away, perhaps the science can move forward.
Hi R,
I know it's tough to think about because a person's past weight isn't modifiable. But look at it this way: it's just a risk factor that affects the probability of negative health outcomes. As always, you can control some risk factors and not others. There are many other factors that you can control, such as your current weight, physical activity level, and diet quality. I don't think there's any reason to feel doomed because you carried excess weight in adolescence, but it might make sense to place a greater emphasis on healthy behaviors than most people.
In the book 'The Obesity Paradox", if I remember right, he doesn't claim more fat decreases your chance of getting heart disease, it decreases your chance of surviving one.
I meant more fat within limits increases your chances of surviving a heart attack.
Hi Peter,
Yes, there is research suggesting an association between higher BMI and better survival post heart attack. I don't think there are very many people who would claim that higher BMI protects against developing heart disease, but there are people who claim that higher BMI is best for overall health, i.e. lower overall mortality risk. This is actually a pretty common idea in the medical world right now, although it remains controversial.
Let me add that I'm not convinced that you're better off with a higher BMI post heart attack. Basically what we see is that the sicker the population, the stronger the confounding in the BMI-health association. I would expect that a post-heart attack population would have a highly confounded relationship between BMI and health outcomes.
Hi Stephan. I looked into this issue from several angles, and wrote about it. In the post below, whose data from Kitava supports your point here very clearly, I suggest an explanation why for modern urbanites carrying some extra body fat can be healthy – “Urbanites may need to carry a bit of extra body fat to be able to have an appropriate intake of micronutrients to maintain their lean body structures in a healthy state.”
http://healthcorrelator.blogspot.com/2013/07/how-can-carrying-some-extra-body-fat-be.html
It's nice when a study confirms something that's intuitive: Being fat is not good for your health.
It is would noting that BMI is a very blunt tool. There are a lot of assumptions that are true in large populations, but would not apply to individuals. Asians tend to have lighter bone structures than Europeans who are lighter than Sub-Saharan Africans. This will tilt the results.
Also, and people are right to point this out, the assumption is that the heavier you are the fatter you are. This is true in general, but can be wildly misleading for individuals. A muscular individual could easily be 'overweight' and still have single digit body fat. A skinny-fat person could be the opposite. Who's at a greater risk for metabolic syndrome? IMO, The skinny-fat person with the nice BMI. If that skinny-fat person started lifting and put on 15 lbs of muscle they would have a *better* long term outlook - not worse IMO.
The correct take-away from this study is that obesity is very bad for you - but that BMI is only applicable to populations - not individuals. A waist vs height measurement (at the belly button) is a much better estimate, but unfortunately much less practical than weight vs. height.
I suspect that waist vs. height would also make the obesity paradox evaporate. Hope someone takes this on.
I am really wondering if that is the best approach to pool the data of thousands or millions of people and come up with an average and recommend that being best for everyone. I would like to see research into the subset of people who did not have increased morbidity or mortality due to being either overweight or underweight. What exactly did protect them? Is it all genetic or certain behaviors, environments, ability to lead a low-stress life, or what else? Epidemiological studies are great to get a first clue of what is going on, but should never be used to make THE SAME recommendation to everyone. There are always individual differences and looking into what drives those differences, finding the actual underlying causes and relationships, is important in my opinion. When I read these studies it always seems like pooling all data on people who ever had an infection and concluding that for most or on average it was beneficial to use an antibiotic. And then concluding that all infections including viral infections should be treated with an antibiotic, which is of course nonsense.
Did these studies control for exercise?
In this meta study we have an increase in mortality for weight gain, unless frequent exercise if occurring, in which case there is nearly no significant relationship between weight gain and mortality, implying that so long as we exercise, weight could be considered a low priority issue (whereas doing exercise has a huge effect at any weight, and more so for higher BMI individuals)
(http://www.onlinepcd.com/article/S0033-0620(13)00155-2/fulltext)
another one for luck:
http://annals.org/article.aspx?articleid=1784291
Adam
"People of Asian/Indian ancestry may be an exception. Their risk level increases more sharply at a lower BMI level."
Given that these two groups account for over half the world's population, perhaps they are not the exception but the norm.
Post a Comment